Dr Norman
Claringbull
Psychotherapist
Counsellor
Psychologist
Former Head of Counselling & Psychotherapy Studies at the University of Southampton; PhD (D. Psychotherapy); MSc (Counselling);
MA (Mental Health); BSc (Psychology) BACP Senior Accredited Practitioner;
UKRC Registered; Prof Standards Authority Registered

The Friendly Therapist
Call or message me now for a free initial telephone consultation
Confidential • Experienced • Based near Southampton
In person or online appointments
Private health insurances accepted
Phone: 07788-919-797 or 023-80-842665

Blog
How CBT works
Posted on July 2nd, 2026
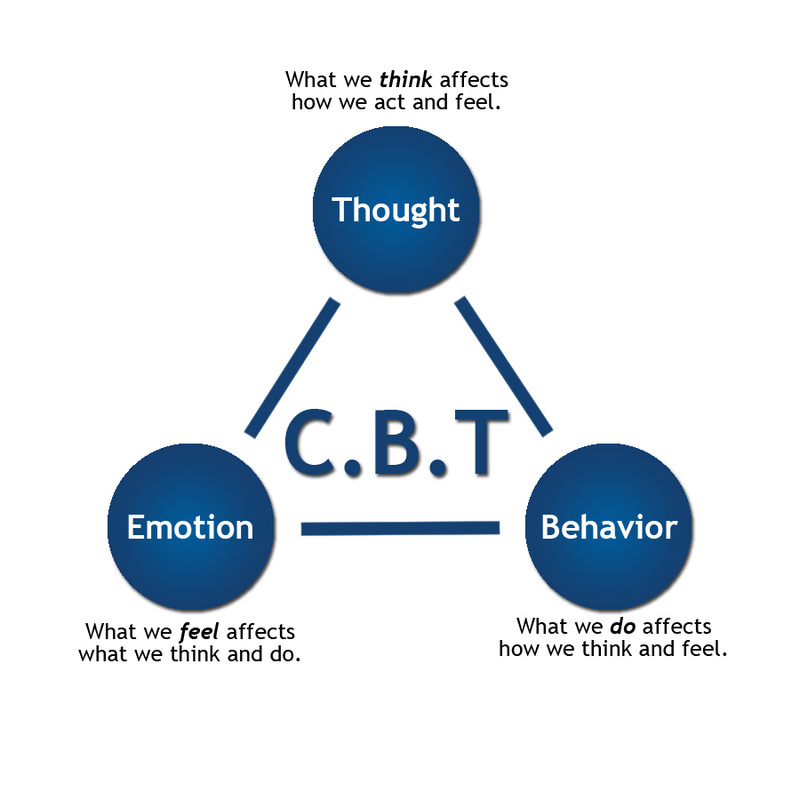
Cognitive-Behavioural Therapy, (CBT), is based on a very simple concept. It is this – Cognitive-Behavioural therapists believe that how we think, (COGNITION) affects how we act, (BEHAVIOUR), and conversely, how we BEHAVE, (actions), affects how we THINK, (cognition). In other words, they claim that it is our individual ways of thinking and behaving that makes each of us who we are and what creates our individual ways of being.
If this is true, then it follows that if we have any psychological problems or emotional difficulties then they must have been caused by psychologically harmful errors in our established ways of thinking and behaving. Therefore, all we have to do in order to ‘cure’ our psychological ‘ills’ is to identify these errors and correct them. Of course, like any ‘Mr Fix It’ we need a work plan and so we need to find out what needs fixing, how to fix it, and how to keep it fixed? When CBT practitioners are trying to help their clients find answers to those three apparently simple questions, they have to keep in mind two important CBT principles
1. The first essential CBT principle this. Events, (each person’s experiences), are not important in themselves, it is how we think about or interpret those events that matters. It is our individual interpretations that make us react in the various ways that we do. For example, seeing someone with a gun is usually frightening, (COGNITION 1), and so we might run away, (BEHAVIOUR 1). However, seeing a police officer with a gun is much less frightening, (COGNITION 2), and so we probably won’t run away, (BEHAVIOUR 2). In other words, it is not the gun itself that is scary but our interpretation of what the gun means, (threatening/non-threatening?), that governs our reaction. It is our perceptions that influence how we think, feel, and act.
2. The second essential CBT principle is this. Feelings, emotions, and thoughts, (COGNITIONS), together with actions, behaviours and physical symptoms, (BEHAVIOURS), are all mutually interlinked and form our individual personality networks. Therefore, any change anywhere, large or small, in our behavioural/cognitive networks will reverberate throughout our entire system and inevitably cause changes.
COGNITIVE ERRORS:
When we get our thinking, (COGNITIONS), wrong then we can cause ourselves all sorts of psychological problems. A core role for a CBT therapist is to try and help clients to discover where their thinking is faulty. Only then can they be helped to put things right. Knowledge is empowering. We can get the wrong idea about ourselves or about what is happening to us in a number of ways. Here are two of the most important sources of error.
i) Negative Automatic Thoughts, (NATs)
We all have them. They are our habitual, (automatic), stereotypical ideas about ourselves: “I’m no good at practical stuff”;“People don’t like me”;“Whatever I do goes wrong”. NATs are all the putting ourselves down ways in which we routinely interpret, (often inaccurately), what goes on in our worlds.
ii) Core Beliefs, (CBs)
These are the fundamental ideas that provide the bedrock of our views about ourselves. A core belief that “I am fundamentally stupid” can underpin such NATs as “I’ll never be able to do crosswords”; “I can’t pass that exam”; “I won’t get that job”. Core beliefs tend to be located in the darker corners of our cognitive ‘storage systems’ and so they are often hard to locate, identify and change.
Either or both of these faulty cognitive processes, (NATs and CBs), contribute to our psychological problems. Their fundamental purpose is to influence how we regularly interpret, (or more accurately misinterpret), life’s events. It is the task of the CBT therapist to help clients to put right any such errors in their thinking. This is a process that psychologists call ‘reframing’.
BEHAVIOURAL ERRORS:
When we get our BEHAVIOURS wrong then that too can harm us. For example, people who have a long-term problem with anxiety may have learned to automatically behave in ways that keep their bodies in a high state of tension, (muscle stress, high pulse rate, over-breathing, and so on). This sort of long-term harmful behaviour will go on to affect long-term thinking, and such a person is often feeling scared and worried, (generalised anxiety, phobias, obsessions, etc.). If they can learn to reduce these levels of harmful behaviour, (de-stress themselves), in some way, (relaxation therapy, yoga, meditating, exercising, etc., etc.), then it is very likely that their fears and worries will lessen as well. In other words beneficial changes in ways of behaving can create beneficial changes in ways if thinking.
AND FINALLY:
All this makes delivering CBT seem very easy. Simply correct bad thinking, (COGNITION), or remedy bad BEHAVIOUR and all will be well. However, in practice doing this is nothing like as simple as it sounds and that is why skilled therapists are needed.
At the beginning of this post, referring to the basic principles of CBT, I did say ‘if this is true’. I put it that way because a lot of psychotherapists, (and very many counsellors), take the view that CBT is a very inadequate response to their patients’ psychological disorders. CBT’s opponents argue that at best it only offers clients symptom relief and that it fails to address their underlying emotional and developmental concerns. Their argument is that even if CBT helps clients to feel better in the short-term, any such benefits are unlikely to be long-lasting. This supposed lack of therapeutic ‘staying power’, CBT’s detractors claim, is because according to them CBT is not ‘proper psychotherapy’.
Personally, I take the view that choosing, or not choosing, to use CBT as a therapeutic tool does not need to be an ‘either/or’ decision. In my psychotherapy practice, CBT and all the other mainstream modes of psychotherapy go hand in hand. That is how I prefer to work with my patients. Each patient is unique and so each patient’s treatment plan is a ‘one-off’. Therefore, I tailor my psychotherapeutic approach, (my treatment plan), to fit each patient’s individual needs. In other words, I give my clients the type of help that they need, when they need it. If they need CBT, then so be it. When they need something different then I give them something different. If that sounds like a ‘best of all worlds’ approach to delivering psychotherapy, then that’s exactly what it is. I’m quite happy to ‘pick and mix’. Whatever works – works!
MINDFULNESS – ANOTHER ‘FLAVOUR OF THE MONTH’?
Posted on June 2nd, 2026
Nowadays, you are a therapeutic nobody if you are not into ‘Mindfulness’. It is psychotherapy’s latest ‘miracle cure’. However, before you get too carried away, don’t forget that just like any other human enterprise, psychotherapy too is subject to the whims of fashion. Up until recently Cognitive Behavioural Therapy was the flavour of the month – now it’s so ‘last year’. These days, Mindfulness is the latest ‘must have’ therapy. Didn’t you know? Are you ‘behind the curve’? Has Mindfulness passed you by? Don’t worry – in a year or two, therapy’s Fashionistas will all be into something else. You can catch up then.
Actually, Mindfulness is not really the bang-up-to-date modern psychological cure-all that its supporters think it is. Like most new ‘wonder therapies’. Mindfulness is only the latest twist on some very old ideas. The fact is that ‘Mindfulness’ is only a new name for some long-established, common-sense, psychotherapeutic techniques, ones that suit some patients and not others. I’ve been using them for years but nobody told me I was being super-trendy.
So, what is Mindfulness? From a psychotherapeutic point of view, it is about encouraging patients to learn how to become very aware of themselves in the present moment whilst at the same time calmly acknowledging and accepting their feelings, thoughts, and bodily sensations. In other words, it is about acquiring the skills necessary to be able to become at ease with all that a patient is experiencing in the immediate here-and-now. Its roots lie in the meditative traditions of ancient eastern religions. There’s nothing in mindfulness that yoga enthusiasts or Buddhism devotees wouldn’t recognise. It’s certainly not new.
Basically, Mindfulness is simply about learning how to become at ease with yourself, about how to become relaxed. There is of course nothing revolutionary about using relaxation as a therapeutic tool. Lots of psychological therapists routinely use Relaxation Therapy, (RT), as a means of treating patients with certain types of anxiety disorders. RT helps patients to learn how to calmly focus on the immediate and then to constructively face their fears. In other words, RT and Mindfulness are simply different sides of the same coin.
In my own practice I use RT because it works, not because it is trendy. Unlike Mindfulness, RT is not based on any spurious ancient, or new-age, belief systems. I’m a scientist and I use scientific principles. The science of RT is based on the biological fact that humans have two major nervous systems. One is the conscious system, That’s the one that we use to think with and to experience emotions and fears. The other is the autonomic system. That’s the one that controls our bodies, (heart rate, breathing, sweating, and other assorted physiological functions). The important biological fact is that these two systems interact with each other. Any ups or downs in one system’s activity levels will cause corresponding movements in the other system. The trick is finding out how to purposely control both nervous systems.
When we feel directly or indirectly threatened we get anxious. These threats can be real or imagined. They can be high intensity and sudden, (a car crash for example); they can be low intensity and long term, (bullying for instance). No matter what sort of a threat it is, when it impacts on us, both the conscious and the autonomic nervous systems rev up and prepare us to deal with it. This is the well-known ‘flight or fight’ response. So, when we become excessively anxious, then clearly these two nervous systems have gone into overdrive. People who suffer from clinically significant levels of anxiety are in a permanent state of heightened conscious and autonomic systems activity. Therefore, when they hit an additional worrying or frightening situation, (real or imagined), their already revved up nervous systems quickly become overloaded. This means that the first key task for the psychotherapist is to help chronically anxious patients to generally reduce their background anxiety levels. The second key task is to help them to learn how to reduce the anxiety engendered by specific real or imagined threats and so not further overburden an already hyper-active system. I have often found that Relaxation Therapy is a very useful way of achieving these two tasks.
Relaxation Therapy is not difficult to apply. It is simply a method of progressively relaxing the body. Initially patients do this under the direction of the therapist. Eventually they learn how to purposefully relax under their own directions. As the body gradually relaxes so too does the mind. Anxieties decrease and panics attenuate – problem solved! On the surface, the methods used to introduce RT to patients might seem similar to those used in hypnotherapy. However, RT is most emphatically not hypnosis. Hypnosis is about a patient temporally surrendering control to the therapist. In direct contrast, the core purpose of purpose of RT is to enable patients to take better control of their own minds, of their own selves. Patients use RT in order to become calmly aware of what’s going on around them; what’s going on in themselves and in the true nature of their own beings. Put simply, they use RT to get their lives into balance in the present and to place tomorrow’s worries where they belong – in the future. The trendies call this Mindfulness. I call it evidence-based psychotherapy.
Anxiety & Stress
Posted on May 3rd, 2026
Anxiety & Stress
Here in the New Forest it looks like spring has sprung – at last. Even looking out over Southampton, we can see some hints of colour and growth. In such happier times it seems almost perverse to start talking about our anxieties and worries. However, we all get anxious; we all get stressed; we have all been there.
The symptoms of anxiety can appear in the mind, (worry, fear, dread, irritability, etc.), or in the body, (palpitations, trembling, sweating, upset tummy, and so on). These days GPs are seeing more and more patients whose anxiety levels are worrying. About 10% of the population suffer from troubling levels of anxiety that are ‘clinically significant’ and about 4% of the population see a doctor about this problem.
Of course not all anxiety or stress is bad for you. It’s natural to feel worried about an urgent problem. On the other hand, if increased anxiety helps us to concentrate better and if increased stress ups our performance then that’s a good thing. Of course when our anxieties get too intense, when they go on for too long, when we find ourselves getting overly anxious or irrationally worried without any obvious cause, when anxiety disrupts our lives, then that’s unhealthy.
So, anxiety, (stress), is neither good nor bad. It is how it affects you that matters. Does it help or does it hinder? Is your level of anxiety OK for you or is it a problem? Anxiety becomes harmful when it starts to overwhelm your ability to cope with life. If stress gets too much to bear, then you can all too easily lose your ability to get by and to manage your life. That’s when you need help
So, how do you get help? The first rule has to be: ‘check with your Doctor’. This is because sometimes what seem to be anxiety symptoms might actually be the result of a physical illness. However, if your doctor tells you that you are generally fit then it is very likely that your symptoms are due to one of the anxiety disorders. That’s when you need to see a psychotherapist or a counsellor. In most cases the available psychological treatments are very effective and most patients start to experience some benefits in about 2 – 4 therapy sessions.
So, don’t put up with anxiety, (stress) – get help – the treatments work!
Remember
- Everybody gets anxious or stressed from time to time – it’s normal
- Low/moderate levels of anxiety or stress can be good for you and improve your performance at all sorts of tasks.
- About 10% of the population experience levels of anxiety that are of ‘clinical concern’. That’s when it is starting to adversely affect their lives.
- When the experience of anxiety is so severe as to disrupt your life, when it diminishes your ability to function, when it starts to take over your being, that’s when you need psychotherapeutic help.
- People suffering from excessive anxiety are said to have an ‘Anxiety Disorder’.
- The Anxiety Disorders include:
- Generalised Anxiety Disorder – the most commonSocial Anxiety Disorder – very commonPanic Disorder – affects a lot of people Agoraphobia – often misdiagnosedObsessive Compulsive Disorder – can be very pervasive Phobias – some are just nuisances, some are very troublesome Acute Stress Disorder – a common, temporary, reaction to trauma Post Traumatic Stress Disorder – less common than you might think
- Anxiety Treatments include:
- Cognitive Behavioural Therapy – helps eliminate/reduce symptomsMedication – helps control the symptomsCounselling and psychotherapy – helps find the root causes Psychological therapy – helps you to cope Self-help training – learn how to manage by yourself Exercise – gets those endorphins flowing
BLOG
Posted on April 7th, 2026
ALL SORTS OF THERAPISTS
There are lots of terms used to describe the health professionals who help people with their emotional, psychological or mental health concerns. Job titles such as counsellor, psychotherapist, psychological therapist, psychoanalyst, psychologist, psychiatrist and many more are all used. The unfortunate fact is that in the UK anyone can call themselves any kind of therapist or ‘ologist’ they like. The exception is the psychiatrists because only they have legally protected titles. With all these names flying about it is not surprising that people often wonder who all these professionals are. What the differences are between them? Who are the genuine article and who are the phonies?
So, how can you tell all these ‘ologists’ apart? Do their professional titles matter? The reality is that all these different titles probably owe more to how any particular therapist was originally trained than they do to actually observable differences in professional practice. After all, research shows us that most experienced therapists are not particularly are overly concerned about professional titles nor do they limit themselves to any given therapeutic approach when responding to their clients’ needs. Therefore, the real answer to the ‘what’s in a name’ puzzle is simple – in practical terms there are no significant differences. Again the exception is the psychiatrists because as medical doctors they can also prescribe medication.
These days, the various sorts of practitioners who offer any of the psychological therapies are often collectively referred to as ‘Talking Therapists’. This term is often also applied to workers in the ‘parallel professions’ such as social work, mental health nursing, probation officers, and so on. When people are using psychotherapeutic techniques, then whatever their backgrounds, they are talking therapists, (even if only temporarily). Of course in these more enlightened times, the psychological therapies increasingly include a lot more treatment methods than just “talking the talk”. Today’s talking therapists encourage people how to self-manage their own conditions by following treatment plans, engaging in practical self-treatment strategies, to get involved with all sorts of psychological interventions. These days the talking therapists don’t just ‘talk the talk’; they “walk the walk” as well.
In addition, people also rightly want to know if they have found genuinely competent and properly qualified counsellors and psychotherapists. The alarming truth is that there are awful lot of quacks out there. Further, there is no way of stopping any of these charlatans causing harm to people by offering them all sorts of weird and wonderful ‘cures’. There seems to be no shortage of psychological snake oil. Therefore, you need to be careful in selecting somebody to trust. How can you make sure that your therapist is the ‘real deal’?
Well, firstly look for people who are fully registered and accredited by one of the main professional bodies. These include the British Association for Counselling and Psychotherapy, The United Kingdom Council for Psychotherapy, the British Association for Behavioural and Cognitive Therapy, or the British Psychological Society? Choosing one of those therapists is much safer for you because they can be disciplined if their standards fall or if they treat their patients unfairly.
Secondly look at their qualifications. Do they have appropriate university level diplomas or degrees in counselling or psychotherapy? Quite simply, a part-time FE Certificate from a local evening college is just not good enough. Be careful here – there are tricksters about. Too many inadequately qualified practitioners give a false impression of themselves by listing all their ‘letters’ even the ones that are irrelevant. An excellent example of this sort of deception comes from the late Dr Marie Stopes the celebrated birth control pioneer. She was never a medical practitioner and her Doctorate was an academic award for research into fossilised plants.
Thirdly, use your common sense. Before making a formal appointment with someone why not have an exploratory chat first, possibly on the phone? Do they sound genuine? Are they willing to answer your questions? Are they prepared to tell you about themselves and about how they work? Are they insured? How experienced are they? Are they professionally supervised? Are they able to refer you on if necessary? Above all, does this person sound like someone you would be happy to talk to? Put simply – do they feel right? If they don’t, then no matter how impressive, (and genuine), their qualifications move on and get somebody else. Go with your instincts – they won’t let you down.
One last thing, If you ever need any help in deciding what to do about selecting the right person and/or the right type of therapy for you then you can always contact me – no charge for free advice – and no, I don’t expect you to come and see me although of course you can if you really want to. I will simply help you choose what’s best for you – that’s what true professionals do – we put patients’ needs first.
ANXIETY & STRESS
Posted on March 25th, 2026
Here in the New Forest, it looks like spring has sprung – at last. Even looking out over Southampton, we can see some hints of colour and growth. In such happier times it seems almost perverse to start talking about our anxieties and worries. However, we all get anxious; we all get stressed; we have all been there.
The symptoms of anxiety can appear in the mind, (worry, fear, dread, irritability, etc.), or in the body, (palpitations, trembling, sweating, upset tummy, and so on). These days GPs are seeing more and more patients whose anxiety levels are worrying. About 10% of the population suffer from troubling levels of anxiety that are ‘clinically significant’ and about 4% of the population see a doctor about this problem.
Of course, not all anxiety or stress is bad for you. It’s natural to feel worried about an urgent problem. On the other hand, if increased anxiety helps us to concentrate better and if increased stress ups our performance, then that’s a good thing. Of course, when our anxieties get too intense, when they go on for too long, when we find ourselves getting overly anxious or irrationally worried without any obvious cause, when anxiety disrupts our lives, then that’s unhealthy.
So, anxiety, (stress), is neither good nor bad. It is how it affects you that matters. Does it help or does it hinder? Is your level of anxiety OK for you or is it a problem? Anxiety becomes harmful when it starts to overwhelm your ability to cope with life. If stress gets too much to bear, then you can all too easily lose your ability to get by and to manage your life. That’s when you need help
So, how do you get help? The first rule has to be: ‘check with your GP’. This is because sometimes what seem to be anxiety symptoms might actually be the result of a physical illness. However, if your doctor tells you that you are generally fit then it is very likely that your symptoms are due to one of the anxiety disorders. That’s when you need to see a psychotherapist or a counsellor. In most cases the available psychological treatments are very effective, and most patients start to experience some benefits in about 2 – 4 therapy sessions.
So, don’t put up with anxiety, (stress) – get help – the treatments work!
Remember
- Everybody gets anxious or stressed from time to time – it’s normal
- Low/moderate levels of anxiety or stress can be good for you and improve your performance at all sorts of tasks.
- About 10% of the population experience levels of anxiety that are of ‘clinical concern’. That’s when it is starting to adversely affect their lives.
- When the experience of anxiety is so severe as to disrupt your life, when it diminishes your ability to function, when it starts to take over your being, that’s when you need psychotherapeutic help.
- People suffering from excessive anxiety are said to have an ‘Anxiety Disorder’.
- The Anxiety Disorders include:
- Generalised Anxiety Disorder – the most commonSocial Anxiety Disorder – very commonPanic Disorder – affects a lot of people Agoraphobia – often misdiagnosedObsessive Compulsive Disorder – can be very pervasive Phobias – some are just nuisances, some are very troublesome Acute Stress Disorder – a common, temporary, reaction to trauma Post Traumatic Stress Disorder – less common than you might think
- Anxiety Treatments include:
- Cognitive Behavioural Therapy – helps eliminate/reduce symptomsMedication – helps control the symptomsCounselling and psychotherapy – helps find the root causes Psychological therapy – helps you to cope Self-help training – learn how to manage by yourself Exercise – gets those endorphins flowing
Hello world!
Posted on March 6th, 2024
Welcome to WordPress. This is your first post. Edit or delete it, then start writing!
BLOGPOST – 2024
Posted on October 18th, 2022
COUNSELLORS AND PSYCHOTHERAPISTS – PROFESSIONALS OR MAGICIANS?
Whenever we contact a professional we usually have a fair idea about what we are likely to get. Doctors doctor, teachers teach, priests preach, and so on. They, and all the other professionals know what they are supposed to do and the public knows what to expect. This is because every profession, every trade, every calling, has its own accepted area of expertise. Lawyers know the law; surveyors know buildings; bankers know finance. They and all the other professional experts know what they are supposed to know. Equally importantly they know what they don’t know. Furthermore, the established professions all require new entrants to be properly trained and to have reached a basic minimum standard before they can start practicing. Can counsellors and psychotherapists say the same? Are they all properly trained, educated, and qualified? Do their customers know what to expect from them.
It seems to me that if practitioners in the psychological therapies, (the so-called ‘talking therapies’), want to be respected as genuine professionals then that respect has to be earned. To begin with they have to be able to answer a very simple question – “what exactly is psychotherapy and/or counselling”? Or, put another way, what is it that counsellors and psychotherapists actually do? What should the public expect of them?
The sad fact is that there is no general agreement within the psychotherapeutic world about what the answers to these apparently simple questions should be. All of the mainstream professions have their core bodies of disciplinary knowledge – their ‘trade secrets’. In the case of the psychological therapies there is no such knowledge base. The problem is that the talking therapies have emerged from a number of discontinuous and conflicting theoretical backgrounds. This means that there is little chance of establishing any professional common ground between the various types of psychological therapists. Therefore, it is unlikely, at least as matters stand right now, that counsellors and psychotherapists could ever agree on a common purpose. They certainly cannot agree on what their trainees should, or should not, be taught. Neither can they agree about what their practitioners should, or should not, be doing. Instead controversy rages, argument abounds, and doctrinal disputes are bitterly fought over.
The story of this on-going, in-house, therapeutic civil war is threaded throughout the history of psychotherapy and counselling. The battle goes on today – no armistice is in sight! The psychological therapies have long been crudely divided into three generic types or ‘Schools’. These distinctions largely remain in place today. This is the root cause of all the rivalries. Firstly there is the Psychodynamic School with its claim that it is our unconscious or instinctual reactions to our developmental experiences that make us what we are. Then there is the Humanistic School with its claim that it is how we deal with our ‘here-and-now’ interpersonal and intrapersonal interactions that define us. Finally there is the Cognitive-Behavioural School with its claim that our personalities depend on our ingrained ways of thinking and behaving. Unfortunately, the adherents of any one of these Schools profoundly reject the arguments of the other two. Equally unfortunately, adherents of each School’s many subdivisions just as passionately reject the stances of their rival subdivisions.
For me, a hard-core scientist, the way to resolve these differences is obvious. Let’s subject all the therapies to some rigorous testing and see what works and what doesn’t. Let’s find some evidence. That is what scientists do! The first obstacle is of course that a significant proportion of counselling’s and psychotherapy’s self-styled ‘professionals’ reject to very notion of scientific enquiry. They claim that therapy is an art and not a science and therefore neither the process nor its outcomes can be, or even should be, codified or measured. So, it seems to me that for those sorts of practitioners, if science is ruled out, it is difficult to see what else they can offer their patients apart from the ineffable. In effect, they are asking their clients to suspend their rational beings and accept instead the power of the unknowable; the indefinable. In other words, they are required to believe in magic. Professional skills are degraded in to hocus pocus. Is the core purpose of counselling and psychotherapy simply to say “abracadabra”? Is that the therapists’ real trade secret?
Actually, as far as the better-educated therapists are concerned, their claim to professional status is based on a much sounder footing. The good news is that properly trained, properly scientific, psychotherapy researchers have produced some good quality evidence. Generally speaking they have found that the mainstream therapies actually work and do so more or less equally. Further research is starting to suggest that there may indeed be some common, or overarching, curative factors permeating most of psychotherapy’s divisions and sub-divisions. This might mean that eventually we could develop a general body of commonly agreed basic disciplinary knowledge that would allow counsellors and psychotherapists to start to call themselves true professionals. Of course that would mean that each therapeutic School’s defenders to give up some of their entrenched positions. However, that is a story for another day. You can find out much more about this issue in my book ‘What is Counselling & Psychotherapy’ – there is a link on my website or you can order it from Amazon.
Finally, please note that in this Blog I began by talking about ‘properly trained, educated, and qualified professionals’. The really scary fact is that anybody, qualified or not, trained or not, can claim to be a counsellor or psychotherapist. The even scarier fact is that some of talking therapy’s main professional bodies continue to admit as members, people whose qualification levels are very questionable. I’ll be discussing that sad state of affairs in my next Blog. I shall be examining the poor quality of therapist training in the UK and revealing how the unqualified charlatans and the underqualified ‘professionals’ deceive their customers.
My book ‘What is Counselling & Psychotherapy’ – follow this link
http://www.amazon.co.uk/What-Counselling-Psychotherapy-Practice-Series/dp/1844453618
BLOG POST – SUMMER 2022
Posted on April 23rd, 2022
CBT – IS IT FOR YOU?
Cognitive Behaviour Therapy – CBT – has been very much the ‘flavour of the month’ in the NHS for some time now. These days, NHS patients with mild to moderate psychological problems are usually referred to a CBT service. This is particularly so in cases of depression or of one of the anxiety conditions. There are two simple reasons why this is so. Firstly, CBT appears to be as effective, (or not), as most of the other types of psychotherapy. Secondly, (and this is the biggie), it is cheap! CBT is cheap to deliver and its practitioners are cheap to train. So, it looks like a win-win situation all round. Well it does until we look a bit closer.
Before we more closely examine CBT let me make one thing very clear. In no way am I against CBT. In the right circumstances it is a very useful type of psychotherapy. It’s a method I very often use with my own patients – but only when it is appropriate. What I am very much against is the over-reliance that today’s NHS puts on to CBT. I am also appalled by the very low levels of training that the NHS requires of its CBT practitioners, especially of its Low Intensity grade of CBT therapists. Now, let’s get back to our closer look at this NHS ‘wonder-therapy’. Is it really so wonderful?
The first point to note is that CBT is only one of the very many types of treatment that properly trained psychotherapists can offer their patients. Obviously no individual practitioner can be an expert in all of these therapies and that is why, like any other profession, psychotherapy has its specialists and consultants. So, if psychotherapists have a wide range of therapies available, (including CBT), why should most NHS patients be directed towards CBT? Clearly patients should be referred for the most suitable type of psychotherapy for their needs, not just CBT for no better reason than it is the cheapest. After all, you wouldn’t expect GPs to prescribe aspirin for everybody simply because it only costs the NHS a few pence to provide. So is CBT a wonder-therapy for all NHS patients or is it really just a wonder-boost for the NHS bean counters.
The second point to take into account is the way in which the NHS trains its CBT therapists. Most of them are graded as ‘Low Intensity Practitioners’. Sad to say, novice Low Intensity therapists do not need to have had any prior experience in mental health work and their training only takes 45 days. Of course, a few of this new breed of low grade therapists, together with a few of the far fewer, (albeit better trained), ‘High Intensity Practitioners’ might, on a personal basis, have acquired additional therapeutic skills from elsewhere. However, the NHS prefers its CBT practitioners to limit themselves to only delivering CBT. They rarely get a chance to use any other skills that they might happen to have. Sadly, most NHS CBT therapists, particularly the Low Level CBT Practitioners couldn’t do so anyway – their training is far too limited.
Thirdly we need to further scrutinize CBT’s actual effectiveness. Clearly, if as is claimed, that CBT is as effective as the other psychotherapies, then do any of its alleged other weaknesses matter. Well yes they do. To begin with, just because a particular therapy apparently works for a particular patient that does not mean that it is the best therapy for that client. After all, an extraction would certainly cure your toothache and do so very cheaply too. However, most dental patients would prefer more modern, more complex treatments even if they cost more. Next, the question of long-term relief versus a short-term quick fix needs to be examined. Many mental health issues, many psychological disorders are of a chronic nature. This means that patients have a life-long, or at or least a very long-term, vulnerability to mental health problems. Without good management these patients are prone to relapse. As CBT is often a short-term fix then it is always possible that one of the more medium / longer term therapies might be more effective in such cases and therefore the true ‘treatment of choice’.
Like many other more extensively trained practitioners, I can, (and do), vary my treatment styles, not just between patients but also within individual treatment programs. In other words I can bring a professional flexibility to my work. Practitioners who only offer one type of psychotherapy, whether that is CBT or anything else, are simply not providing anything like the comprehensive service that today’s complex-needs clients require. Put bluntly, they are failing their clients.
In sum what I am saying is that CBT is an excellent form of psychotherapy but only at the right time and in the right pace. However, it is not the super cure-all that the NHS would have us believe. In my next blog I’ll tell you more about how CBT works. I’ll even let you into a secret. For many patients, using a professional CBT therapist is not always necessary – DIY can be pretty effective too. Next time I’ll tell you how.

BLOG POST – SPRING 2022
Posted on November 23rd, 2021
DANGER – ‘THERAPISTS AT WORK!’
For lots of people, feelings and sentiments are messy, embarrassing, and best avoided. When emotions are running high then it’s usually easier to send for the ‘ologists’ than to deal with the sufferers at first hand. That’s why the general public relies on therapists to mop up all that emotional ‘goo’. As a result, modern day counsellors and psychotherapists are all too often used as society’s emotional refuse collectors.
It’s bad enough that society thinks that these modern day, therapeutic ‘Fairy Godmothers’ can magic away unwanted psychological pain. What’s even worse is that all too many counsellors and psychotherapists actually believe it too. For example, whenever there is a particularly tragic event, a murder in a school say, or perhaps a terrorist attack, the news services all solemnly announce that counsellors are in attendance. Now any properly trained psychologist or psychotherapist knows that not only is such an immediate on-site presence irrelevant, but that it can actually be harmful. The problem is that all too few therapists are properly trained. So in they go, ‘saving the world’, smugly blissful in their ignorance. There are other appropriate psychological interventions that do help in the immediate aftermath of emergency situations. These include psychotherapeutic ‘First Aid’ and psychological trauma triage. Unfortunately, very few counsellors and psychotherapists have even heard of these techniques much less ever learned how to use them.
However, this is not the only area in which the ill-trained majority of the Talking Therapy World’s practitioners rush in where angels fear to tread. That’s because to them, counselling and psychotherapy are always ‘good things’. Therefore, the therapy trade’s practitioners, with their allegedly non-judgemental, multi-cultural, ethos, must be generally beneficial to their customers, (or so they claim). So, whatever the problem, there go the therapists bringing their own special brand of succour to the emotionally wounded, (or so they think). As ever, the road to hell, including psychotherapy’s own version of hell, is paved with good intentions.
However, what most therapists don’t realise is that far from being socially neutral, judgementally neutral, and value-free, the practice of counselling and psychotherapy over the last 50 years or so has actually been an affirmation of a specific socio-political attitude that is still prevalent amongst an intellectually liberal elite in western society. This is the self-centric, self-actualising, way of being that underpins a ‘me, me, me’ view of the self and the world that has been prevalent amongst the ‘right-on’ generation from the 50s onwards. Counselling’s great guru, Carl Rogers certainly has such a lot to answer for.
This ‘me first’ generation, the so-called ‘baby boomers’, found it intellectually convenient to invent a way of ordering society, (and supposedly curing its emotional ‘ailments’), that fitted in with their own belief systems, (or prejudices). They also invented their own Orwellian ‘Newspeak’, (Political Correctness), to supress any alternative viewpoints. So, in this allegedly freer modern society, it seems that only approved of ideas are permissible. Alternative viewpoints should not even be listened to. Far from being intellectual libertarians, today’s super-sensitive right-thinkers happily no-platform the opposition in order to save their own delicate beings from being offended.
So, you don’t think all us super-empathetic, super caring, therapists can be bigoted like that? We can’t be biased or dogmatic? Just go along to any group of counsellors or psychotherapists talking about their work. You will see what I call ‘the noddies’. They will all be nodding approvingly at any statement that fits in with their group-think and looking uncomfortable should any renegades question any of their core beliefs. The fact is that all too many of practitioners in the talking therapies are dangerously undereducated. Most of their training consists of being inculcated with a lot of professional ‘does and don’ts’. Unfortunately, therapist education is mostly normative. It is very rarely formative. Critical thinking is not encouraged. How could it be? After all, most of their instructors don’t even begin to understand the concept of academic criticality and they recoil at even the idea of scientific methodology. How could they? They too are the products of inadequate training.
Is there a way out of this intellectual backwater, at least as far as the talking therapies are concerned? Well yes, but first the psychotherapeutic professions must go through the same healing process that they encourage in their customers. Firstly, deal with denial. Admit that all too many practitioners are currently inadequate for the task. Secondly, determine what is wrong. In my view the core problem is the sheer educational inadequacy of therapist training and therapist trainers. Put bluntly, in the purist sense of the word, all too many of them are educationally defective and intellectually undeveloped. Thirdly, make some serious changes. Doing that, I believe, means establishing some new and upgraded professional standards. These should include establishing a minimum educational requirement of BSc, (not BA), level training for counsellors and an MSc, (not MA), level training for psychotherapists. There should also be a recognised post-qualification licensing procedure.
Of course, my proposals for upgrading counselling and psychotherapy’s professional standards are all ‘pie in the sky’ at present. So what can Joe and Jill Public do about finding a properly trained and qualified therapist? How can they find somebody who actually knows what they are doing? I’ll tell you all about that in my Spring Blog.
BLOG POST – AUTUMN 2021
Posted on August 27th, 2021
DEPRESSION – CAUSES AND CURES:
Depression is not the same as feeling downhearted or sad. We all get seriously fed up or feel in a really down mood from time to time. That’s not depression; that’s life. However, sometimes those low moods won’t go away and we don’t bounce back. If those low moods start to seriously affect our lives, to cause us to behave noticeably differently, to interfere with our usual day-to-day functioning, then that’s when psychologists start to consider that we might be suffering from clinically significant depression.
Depression is a very common psychological disorder. Probably about one in four of the UK population develop worrying levels of depression at some time or other in their lives. It’s very likely that about one in ten of the people sitting in your local GP’s waiting room today are taking anti-depressants. There are very few people who have not either been depressed themselves or who do not have a family member or a close friend who has been so afflicted. However, depression is all too often a ‘secret illness’ and its sufferers don’t like to let other people know about their condition. That’s because, even today, mental ill-health still carries a social stigma. So what causes depression and what should sufferers do about it?
Depression in its clinical sense usually arises when life’s problems overwhelm us. What these problems are, and how they affect us will vary from person to person. They don’t have to be huge, ‘blockbuster’ worries. A lot of little things, occurring over a long time can be just as depressing as some serious, one-off, blows to our way of being. Some theorists wonder if depression has a genetic component. Put simply, some people think that’s just how you are made. Other theorists wonder if depression has a nurturing component. In other words, are you feeling low because, in your experience, life is pretty naff.
Lots of different psychotherapeutic theorists have lots of different, (and competing views), about the causes of depression. They also have lots of views about the best ways to treat depression. However, most practitioners would agree that the core component of depression is Anhedonia. This is an emotional state in which the sufferer generally loses interest in life, has little motivation, feels the future is hopeless, and is usually unable to experience pleasure. Such a person is generally emotionally flat. Nevertheless, whatever, the cause, people with depression need help. So, what can be done for them? What can they expect from the mental health professionals?
In the UK the generally accepted approach to depression is to deliver treatment in a number of steps.
Step 1 – mild depression – is generally best treated by doing nothing. Left alone, most mildly depressed patients spontaneously recover within six months. In these sorts of cases therapists must be careful not to ‘over-therapise’ because doing so might well make things worse. However, basic-level supportive counselling can sometimes help with the healing process. It can also be the case that elementary CBT might prove useful to such sufferers. This usually involves something easy like providing patients with some basic information about their condition and teaching them some simple steps that they can take to help themselves.
Step 2 – mild to moderate depression – this is usually more actively treated. Doctors will usually prescribe an antidepressant and psychotherapists normally offer more detailed and more intensive psychotherapeutic interventions and CBT treatments. For most people a treatment plan that combines pills, talking, and self-management skills training is generally the most productive way forward.
Step 3 – severe depression – requires a more intensive approach, both from the medics and the therapists. A referral to a psychiatrist or the local Community Mental Health Team is usually indicated. At this stage, adopting a more powerful medication regime might be necessary. Again, psychotherapy is an important part of the overall treatment plan, even in cases serious enough to require hospitalisation.
So there you have it, depression is common, it can be crippling but it does not have to rule your life. If it strikes, don’t suffer in silence – get help – it works.